Making sense of consent and health records in the digital age
May 8, 2016 § 2 Comments
There are few more potent touchstones for the public than the protection of their privacy, and this is especially true with our health records. Within these documents lies information that may affect your loved ones, your social standing, employability, and the way insurance companies rate your risk.
We now live in a world where our medical records are digitised. In many nations that information is also moving away from the clinician who captured the record to regional repositories, or even government run national repositories.
The more widely accessible our records are the more likely it is that someone who needs to care for us can access them – which is good. It is also more likely that the information might be seen by individuals whom we do not know, and for purposes we would not agree with – which is the bad side of the story.
It appears that there is no easy way to balance privacy with access – any record system represents a series of compromises in design and operation that leave the privacy wishes of some unmet, and the clinical needs of others ignored.
Core to this trade-off is the choice of consent model. Patients typically need to provide their consent for their health records to be seen by others, and this legal obligation continues in the digital world.
Patient consent for others to access their digital clinical records, or e-consent, can take a number of forms. Back 2004, working with colleagues who had expertise in privacy and security, we first described the continuum of choices between patients opting in or out of consent to view their health records, as well as the trade-offs that were associated with either choice [1].
Three broad approaches to e-consent are employed.
- “Opt Out” systems; in which a population is informed that unless individuals request otherwise, their records will be made available to be shared.
- “Opt in” systems; in which patients are asked to confirm that they are happy for their records to be made available when clinicians wish to view them.
- Hybrid consent models that combine an implied consent for records to be made available and an explicit consent to view.
Opt in models assume that only those who specifically give consent will allow their health records to be visible to others, and opt out models assume that record accessibility is the default, and will only be removed if a patient actively opts-out of the process. The opt-out models maximises ease of access to, and benefit from, electronic records for clinical decision making, at the possible expense of patient privacy protections. Opt-in models have the reverse benefit, maximising consumer choice and privacy, but at the possible expense of record availability and usefulness in support of making decisions (Figure 1).
 Figure 1 – Different forms of consent balance clinical access and patient privacy in different proportions (from Coiera and Clarke, 2004)
Figure 1 – Different forms of consent balance clinical access and patient privacy in different proportions (from Coiera and Clarke, 2004)
All of the United Kingdom’s shared records systems now emply hybrid consent models of one form or another. Clinicians can also ‘break the glass’ and access records if the patient is too ill or unable to consent. In the US a variety of consent models are used and privacy legislation varies from state to state. Patients belonging to a Health Maintenance Organisation (HMO) are typically deemed to have opted in by subscribing to an HMO.
How do we evaluate the risk of one consent model over others?
The last decade has made it very clear that, at least for national systems, there are two conflicting drivers in the selection between consent models. Those that worry about patient privacy and the risks of privacy breeches favour opt-in models. Governments that worry about the political consequences of being seen to invade the privacy of their citizens thus gravitate to this model. Those that worry about having a ‘critical mass’ of consumers enrolled in their record systems, and who do not feel that they are at political risk on the privacy front (perhaps because as citizens our privacy is being so rapidly eroded on so many fronts we no longer care) seem comfortable to go the opt-out route.
The risk profiles for opt in and opt out systems are thus quite different (Figure 2). Opt-out models risk making health records available for patient’s who, in principle, would object to such access but have not opted out. This may because they were either not capable of opting-out, or were not informed of their ability to opt-out.
For opt-in models, the greatest risk to a system operator is that important clinical records are unavailable at the time of decision-making, because patients who should have elected to opt-in were neither informed that they should have a record, or were not easily capable of making that choice.
Other groups, such as those who are informed and do opt-out, may be at greater clinical risk because of that choice, but are making a decision aware of the risks.

Figure 2: The risk profiles for opt-in and opt-out patient record systems are different. Opt-out models risk making records available for patients who in principle would object to such access, but were not either capable or informed of their ability to opt-out. For opt-in models, the risk is that important clinical records are unavailable at the time of decision making, because patients who should have elected to opt-in were neither informed nor capable of making that choice.
Choosing a consent model is only half of the story
In our 2004 paper, we also made it clear that choosing between opt-in or out was not the end of the matter. There are many different ways in which we can grant access to records to clinicians and others. One can have an opt-in system which gives clinicians free access to all records with minimal auditing – a very risky approach. Alternatively you can have an opt-out system that places stringent gatekeeper demands on clinicians to prove who they are, that they have the right to access a document, that audits their access, and allows patients to specify which sections of their record are in or out – a very secure system.

Figure 3 – The different possible functions of consent balance clinical access or patient privacy in different proportions. The diagram is illustrative of the balances only – thus there is no intention to portray the balance between access and privacy as equal in the middle model of e-Consent as an audit trail. (From Coiera and Clarke, 2004)
So, whilst we need to be clear about the risks of opt in versus opt out, we should also recognise that it is only half of the debate. It is the mechanism of governance around the consent model that counts at least as much.
For consumer advocates, “winning the war” to go opt-in is actually just the first part of the battle. Indeed, it might even be the wrong battle to be fighting. It might be even more important to ensure that there is stringent governance around record access, and that it is very clear who is reading a record, and why.
References
- Coiera E and Clarke R, e-Consent: The design and implementation of consumer consent mechanisms in an electroninc environment. J Am Med Inform Assoc, 2004. 11(2): p. 129-140.
What should a national digital health system look like?
May 1, 2016 § Leave a comment
What is the role of government in contributing to the nation digital health infrastructure? That is not an easy question to answer. Every nation has its own specific variant of a health system, with different emphases on the public or private, on central government intervention or laissez-faire commerce. I have in earlier blogs made the point that, despite these differences in national systems, we now collectively have enough experience that we cannot ignore the evidence when crafting national strategies.
Back in 2009, when I explored the implications of these structural differences for government, I came to the conclusion that digital health needed a ‘middle out’ governance model, rather than top-down or bottom-up approaches to strategy. One consequence of the thinking in that paper was that I formed a view that we did not need a centralised national summary care record – a view which left me with fewer friends in government than I used to have! I was only trying to be helpful …
With a new Australian Digital Health Agency, it is now a good time to revisit these questions, to learn from the past, and to come together as an informatics and e-health community, and give ourselves the best possible shot at getting digital health right.
Digging through my papers recently, I came across this briefing paper I wrote for the Secretary of Health in 2008 – well before the middle out and summary care record papers. It was a time when Facebook was in the ascendancy, so I used the term ‘Healthbook’ to portray my ideas for a distributed, federated digital information system. Maybe now is a good time to revisit its spirit, if not the technical details?
‘Healthbook’ – the consumer as catalyst for the creation of a national ehealth infrastructure
E. Coiera, 2 May 2008
Briefing paper to DOHA
Current situation
Australia like many nations is struggling to identify a strategic approach to creating a health information infrastructure that is technically feasible, low risk, and affordable.
The current proposal for a national shared electronic health record (SEHR), presumes a centralised, potentially monolithic, structure, where every Australian has a health record summary stored for them, to facilitate health care provision. The mental model is similar to English NHS’ system, which has cost billions of pounds to implement, and has experienced significant technical and implementation challenges on the way. If Australia were to take a similar centralised approach to the SEHR, then it too would cost several billion dollars, presuming our cost structures are similar to the English NHS, and face its own technical risks. And after investing that money we are locked into ageing technologies that require continued significant investment. Implementation starts, but it never ends.
A second disadvantage of beginning with a centralised SEHR is that it demands ‘delayed gratification’. There is massive up front investment, substantial pain within the health jurisdictions during implementation, with benefits only arriving after many years, and little for consumers to see or appreciate despite the large sums of money being invested. It also draws resources away from other cheaper, but potentially higher value, elements of the eHealth infrastructure, specifically decision support technologies, which have great capability to reduce harm, improve safety, and deliver efficiency gains through more evidence-based use of investigations and therapeutics.
A different way
An alternative approach has emerged. Imagine that, rather than waiting 5-10 years for a ‘centrally planned’ SEHR (that is what it may take) we achieve many of the same goals in less than 5 years, at significantly less cost to government, in a market-driven and industry lead way, growing organically and flexibly, rapidly adopting technological innovation, and potentially building up new export industries for Australia’s IT industry. Imagine also if this new way had strong support from consumers, because it was all about them and their health care, and not about putting in expensive ‘backroom’ technologies they will never see.
There are three elements to this approach:
1 – The shareable record can be consumer rather than health service focussed: Utilising the resources of private industry, consumer demand for access to their record, personal health records are emerging as a major new business sector. The strongest evidence for this is the move by two of the largest IT companies into this space. Microsoft has made its first major step into healthcare with its HealthVault product, and Google Health is emerging as their main competitor. Both offer consumers a service to store their personal health information, and to make it accessible to health providers with consumer consent.
In the US many large health service organizations have many millions of their patients using locally developed personal health records, for example the VA hospitals, and Partners. Similar activities are underway here with smaller start-up companies e.g. myvitals.com. Expect a flurry of such companies to appear locally, or arrive from overseas, over the next 12 months.
There is much to be commended about personal health records, but there are also some major limitations, including – the potential for the consumer created record to be of poor quality or perceive to be so by clinicians, the lack of interoperability between different systems, the consequent locking in of one’s records to a single vendor, the poor connectivity between health service provider records and personal health records, the significant risk that personal health information may be used for secondary and commercial purposes, and for Australian’s, the very real risk that core national IP – the health records of all Australians, is stored overseas – resulting in a massive transfer of information and wealth overseas.
2 – The rise of social computing. While there has been talk of the internet being an online community since the mid ‘90s, only in the last 2 years has this really taken off, with Facebook, My space and others providing a sophisticated social networking experience that has caught the imagination of the average consumer, trained consumers in sophisticated information sharing strategies, and developed software to support this. Consumers are now comfortable to carry out many of their most personal transactions on the web, from banking, to finding partners and socializing. Blogging has created a generation that is far more comfortable in sharing their personal information than any before.
3 – The continuing rise of search. Google and its competitors continue to prosper. Health information is amongst the top two categories of information searched for. Consumers want information about their health, and continue to turn more to the Internet for that information.
Putting these three together it may now be possible for private industry to create information services that challenge the centralized monolithic SEHR model, and create a rich and flexible ehealth infrastructure on the way.
The idea of a facebook for health (or ‘healthbook’) is fairly straightforward – it is a web space where you manage your health information and access health information services, in the same way that your internet banking account is the place you manage your wealth e.g. looking at account balances, paying bills, transferring funds. There will be many competing ‘healthbook’ systems provided by industry, and we can expect companies to be offering consumers at least some or all of the following services:
- A personal health record, where you enter your own health information;
- Access to health information e.g. search engines, local guidelines, drug information, health leaflets;
- A social computing environment in which a personal health record and information can be shared amongst family, friends, clinicians, and groups;
- Links to a selected subset of health providers, allowing them to see personal health records, exchange messages (reminders, appointments, results, health messages), and maybe allow you to see some of their records about you e.g. a division of GPs might offer this service, or a private health insurer may negotiate with health service providers to offer this to their clients.
It is important to emphasise that we are not saying that the personal record now becomes the shared health record – it cannot and should not – but that the links to different clinical record systems we might find in a ‘healthbook’ effectively provides the first stage in shared access to clinical records. While such systems will grow organically, and possibly quite quickly, there are several missing pieces and some concerns that need to be addressed, including:
- Message exchange and access to your records stored by the public hospital system
- Message exchange and access to your records stored by other health services not part of the particular online consortium you join.
- Interoperability between systems, allowing consumers to take their personal health information, and linked messages and records, to a different provider.
- Protections for Australian health information going overseas and being exploited for secondary commercial purposes.
- Accreditation of healthbook providers to ensure clinical service providers and patients are comfortable in making their clinical records available via them.
If issues such as these were addressed quickly, we may in Australia be creating business conditions not yet operating anywhere else in the world, and create an opportunity for our local IT industry to corner or at least become highly competitive in a new business clearly destined to become the single largest information technology market.
It thus seems entirely feasible for government to choose not to invest in a monolithic national e-health infrastructure, but foster competition and rapid expansion of a web and business driven infrastructure. Government creates appropriate protections for the community and their personal information while supporting high quality and safe clinical care. Government is a key enabler, working with the professions and individuals to identify incentives and provides critical missing elements needed to fast track this world, including regulation, legislation, investment in making jurisdictional systems interoperable, provision of public knowledge and information sources, and investment in evaluation and research to drive evidence-based innovation.
What might happen next
If government steps in to address some of these barriers to fully interconnecting consumer-based personal health records, we could imagine three stages in the evolution of our national eHealth infrastructure:
Stage 1 (next 2 years) – Personal health record systems available and taken up by a few Australian. Some offer access to knowledge services e.g. Healthinsite; some service providers band together to allow their records to be linked to these systems and for messages to be exchanged between providers and consumers within this system. Records might be shareable within these restricted health service organizations. Standards are being developed by NEHTA, ISO and Standards Australia, and industry and the jurisdictions are moving to comply with these as they install eHealth systems.
Stage 2 (2-3 years) – Messaging standards and unique and secure IDs for every Australian (the UPI) are in place and allow communication between providers and any standards compliant ‘healthbook’. Record portability legislation encourages innovation and competition and avoids monopoly outcomes (similar to mobile telephone number portability, where a consumer can take their phone number and address book from one Telco handset and swap them to a different one). Some state jurisdictions and primary care divisions provide standard secure web interfaces to any accredited private system, and consumers chose to link to their records in these systems, if they are aware that they are able to. When viewing linked records they appear in non-standard ways, dependent on the structure of the local system the record sits on. 10% of Australians have a ‘healthbook’ page, with international IT companies amongst the major players, but Australians may end up trusting their health providers and government with their private information, so the biggest user base may be found with Divisions of general practice, or private health insurance companies. Many other players jockey for dominance.
Stage 3 (3-5 years) – Interoperability standards have allowed any accredited record provider to provide a discoverable web service, so that any healthbook can access these records, with consumer permission. This means when you create your new healthbook account and put in your UHI, the system will find all the records associated with your care that are on the web, and ask you if you want to link them in. When records are browsed from within a consumer space, they have a uniform appearance. So, irrespective of which company’s ‘Healthbook’ you use, a clinician can always find the information they want in the same place, by selecting the ‘common user interface’ option. It is possible to extract elements of provider records into a personal health record manually or automatically. For example, you can extract medication lists, test results, or allergies from your GP system into your personal health record.
For those who choose it, their treating clinician may decide which data gets extracted from the clinical record into the personal summary record. For Australians who are not interested in using a private system, or are unable to do so, a ‘vanilla’ personal health record is made available, possibly via the jurisdictions, that allows a provider to see other linked records for a given patient, with a patient’s consent. Local Australian companies provide the back end service to consumer health sites, with the front end run by large health delivery organizations e.g. public hospital systems, and private insurers. International IT companies provide some of the core technologies underpinning these systems but the data is stored in Australia, protected by legislation from going offshore, or even analyses of the data going offshore.
The Role of government
Government has a role to:
- Facilitate – through standards activities (NEHTA) and early investment for industry development and research. For example COAG may wish to provide seed funding for 2-4 large-scale implementations e.g. requiring each consortium to include a public hospital system, a primary care organization, and for some % of the industry membership to be locally based. This attracts industry to invest, and creates a competitive climate in which innovation is focussed on delivering to the consumer as the main customer. It should be clear investment is for start up and that all programs need to be self-funding at the end of the projects. There may be incentives for meeting subscription and transaction rate milestones, and for health services incentives for meeting outcome targets e.g. preventative health activities. There may be penalties for failure to deliver, including withholding of payments should benchmarks not be met. There should be some key deliverables that we expect of out any such consortia, including:
- Working with standards organizations like NEHTA, they should agree on a working record portability standard and mechanism, that allows a consumer to extract their personal health record, provider messages, links to clinical records, and any other information such as a future shared health record, and transfer it to another provider;
- Consortia should demonstrate interoperability between each other for record mobility between consortia, and for messaging between providers and different consortia.
- Working with standards organizations, the consortia should agree on a default ‘common user interface’, which provides a uniform way of accessing linked records, messages, and patient data for clinicians and consumers. There is no obligation to use this interface as different systems will want to ‘value add’ and provide better user experiences for their customers. We want to ensure that clinicians will only need to learn how to access healthbook records once, and always find the information they need in the same place every time – for safety as well as efficiency reasons.
- Demonstrated use of a unique personal identifier like the UHI, ensuring secure and safe creation of new accounts, protection of personal information, and ease of access in clinical situations.
- Demonstrated security and consent mechanisms so that consumers feel safe using these systems.
- Protect – the privacy of individuals, and the national IP – through legislation, and where appropriate accreditation. Consumers will need record portability and not be locked into one vendor, so legislation should allow for consumers to extract their digital records from any one vendor and move to another. Consumers and providers will want to know that healthbook systems are accredited before records are linked into them, and that accreditation ensures that records made available this way are not used for any purpose other than clinical care, and only with the consent of consumers.
- Evaluate – We need benchmarks for this program, both in terms of uptake by citizens, as well as adoption rates, usage and benefits. Evaluation programs for benefits are best run by independent organizations, and this is a clear role for academic institutions.
- Ensure Access – Ensuring all citizens and health service providers have access via a decent broadband system, and for those citizens who choose not to actively be engaged, or are unable e.g. infirm, elderly, then create an option of clinician or health service managed e-services where the consumer gives permission for their ‘healthbook’ to be created for them. Facilitate early adoption by service providers with an incentives program (e.g. to make practice records linkable to commercial systems).
- Innovate – We want Australian industry to have access to new ideas and IP to make them competitive with the US industry in particular, and there is a clear opportunity to support Australian R&D and innovation with targeted support for eHealth innovation programs.
- Participate – where jurisdictions control medical content such as records or knowledge resources (Healthinsite, service or provider directories), make these available and interoperable with private sector systems. Where government has a specific duty to individuals such as military personnel, provide or auspice services available to citizens e.g. military personnel may have records that cannot be linked for security reasons to commercial systems, so a military system might be needed, which links to all public records, but remains secure.
Appendix – Some benefits and ideas worth capturing at this stage
Benefits of this approach
- A better informed, better engaged population
- A transition plan to implementing SHER functions, not a ‘big bang’ centralised SHER, which is a single point of failure if things go wrong.
- Technical and investment risks are lower, as the elements government may want to invest in e.g. standards, making jurisdictional records compliant, and messaging are all required under the monolithic SEHR model too. So, if the consumer-drive model does not work, government can in the future elect to step in and can complete the ‘last mile’ e.g. with health information exchanges.
- Most of the implementation risk is borne by private enterprise
- A shift to preventative healthcare, as consumers build for possibly the first time a place where they actively manage their healthcare, and receive targeted messages and support.
- Safer care – driven by consumer benchmarking and rating, the use of consumer decision support systems, easier interaction with clinicians via messaging, a shareable record that allows clinicians to see the bigger clinical picture.
- Support for the Australia it industry and research community to become a world leader in a market that is highly lucrative – if there is to be a new company that becomes the Google of healthcare, why could it not be an Australian company?
Ideas
- Use the healthbook to send reminders for vaccinations, screening tests, routine check ups.
- Support for healthy journeys e.g. parents with young children accessing information at crucial child development stages, and possibly linking up with the community 1-stop shop proposal by government.
- If every high school student has a computer why can’t they use ‘healthbook’ applications to manage their exercise and eating regimes, by providing a online social environment where quality information is shared, groups can form e.g. how to cope with anorexia or obesity, providing information and social support?
- Support for more targeted, efficient access to services e.g. by providing consumers health service directories, similar to ‘choose and book’ in the NHS, with the ability to identify providers, and make appointments. Especially valuable for rural and remote citizens to identify services that might be available to them outside of local area.
- Consumer based benchmarking of services – similar to Amazon star rating for books (this will happen anyway – best to support it being as informative and balanced as possible).
Four futures for the healthcare system
February 20, 2016 § 1 Comment
That healthcare systems the world over are under continual pressure to adapt is not in question. With continual concerns that current arrangements are not sustainable, researchers and policy makers must somehow make plans, allocate resources, and try to refashion delivery systems as best they can.
Such decision-making is almost invariably compromised. Politics makes it hard for any form of consensus to emerge, because political consensus leads to political disadvantage for at least one of the parties. Vested interests, whether commercial or professional, also reduce the likelihood that comprehensive change will occur.
Underlying these disagreements of purpose is a disagreement about the future. Different actors all wish to will different outcomes into existence, and their disagreement means that no particular one will ever arise. The additional confounder that predicting the future is notoriously hard seems to not enter the discussion at all.
One way to minimize disagreement and to build consensus would seem to be to have all parties come to a consensus of what the future is going to be like. With a common recognition of the nature of the future that will befall us, or that we aspire to, it might becomes possible to work backwards and agree on what must happen today.
Building different scenarios to describe the future
There seem to be two major determinants of the future. The first is the environment within which the health system has to function. The second is our willingness or ability to adapt the health system to meet any particular goal or challenge. Together these two axes generate four very different future scenarios. Each scenario has a very different set of challenges to it, and very different opportunities.
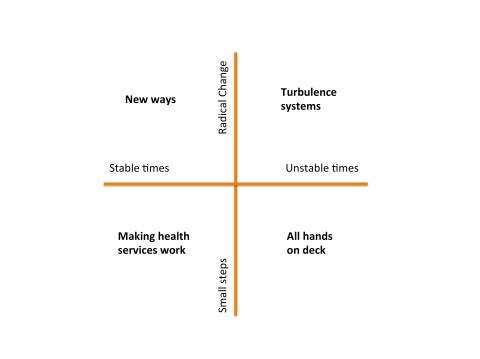
Making Health Services Work: In this quadrant, we are blessed with relatively stable conditions, and even though our capacity or will for change is modest, we can embark on incremental changes in response to projected future needs. We focus on gentle redesign of current health services, tweaking them as we need. The life of a heath services researcher is a comfortable one: no one needs or wants a revolution and there is time and resource enough to solve the problems of the day.
New Ways: Despite forgiving and stable times, in this quadrant we have an appetite for major change. Perhaps we see major changes ahead and recognize that incremental improvements will be insufficient to deal with them. Maybe we see future years with demographic challenges such as clinical workforce shortages and the increasing burden of disease associated with an ageing population. Consequently, more radical models of care are developed, evaluated and adopted. Rather than simply retro-fitting the way things are done, we radically reevaluate how things might be done, and envisage new ways of working, and conceive new ways to deliver services.
Turbulence systems: The risk of major shocks to the health system are ever present, including pandemics, weather events of ‘mass dimension’ associated with climate change, and human conflict. It is possible to make preparations for these unstable times. We might imagine that we set about to design some capacity for ‘turbulence’ management into our health services. Such turbulence systems would help us detect emerging shocks as early as possible, and would then reallocate resources as best we can when they arrive. The way that global responses to disease outbreaks has rapidly evolved over the last decade shows what is possible when our focus is on shock detection and response. Similar turbulence systems are evolving to respond to natural disasters and terrorism – so there are already models to learn from. In this quadrant then, we redesign the health system to be far more adaptive and flexible than it is today, recognizing that the future is not just going to be punctuated by rare external shocks, but that turbulence is the norm, and any system without shock absorbers will quickly shatter.
All hands on deck: In this scenario, health services receive major shocks in the near future, and well ahead of our ability to plan for these events. For example a series of major weather events or a new global pandemic could all stretch today’s health system beyond its capability to respond. Another route to this scenario in the long term is to not prepare for events like global warming or infectious disease outbreaks or an ageing population, and because of disagreement, underinvestment or poor planning, we do nothing. If such circumstances arrive, then the best thing that everyone in the health system can do is to abandon working on the long term, and apply our skills wherever they are most needed. In such crisis times, researchers will find themselves at the front lines, with a profound understanding and new respect for what implementation and translation really mean.
Picking a scenario
Which of these four worlds will we live in? It is likely that we have had the great good fortune over the last few decades of living in stable and reactively unambitious times, tinkering with a system that we have not had the appetite to change much. It seems likely that instability will increasingly become the norm however. I don’t think we will have the luxury of idly imagining some perfect but different future, debating its merits, and then starting to march toward it. There will be too much turbulence about to ever allow us the luxury of knowing exactly what the right system configuration will be. If we are very lucky, and very clever, we will increasingly redesign health services to be turbulence systems. Even if the flight to the future is a bumpy one, the stabilizers we create will help us keep the system doing what it is meant to do. ‘All hands on deck’ is the joker in the pack. I personally look forward to not ever having to work in this quadrant.
[These ideas were first published in a paper my team prepared back in 2007, and since it first appeared, the turbulence has slowly become more frequent …]
Evidence-based health informatics
February 11, 2016 § 6 Comments
Have we reached peak e-health yet?
Anyone who works in the e-health space lives in two contradictory universes.
The first universe is that of our exciting digital health future. This shiny gadget-laden paradise sees technology in harmony with the health system, which has become adaptive, personal, and effective. Diseases tumble under the onslaught of big data and miracle smart watches. Government, industry, clinicians and people off the street hold hands around the bonfire of innovation. Teeth are unfeasibly white wherever you look.
The second universe is Dickensian. It is the doomy world in which clinicians hide in shadows, forced to use clearly dysfunctional IT systems. Electronic health records take forever to use, and don’t fit clinical work practice. Health providers hide behind burning barricades when the clinicians revolt. Government bureaucrats in crisp suits dissemble in velvet-lined rooms, softly explaining the latest cost overrun, delay, or security breach. Our personal health files get passed by street urchins hand-to-hand on dirty thumbnail drives, until they end up in the clutches of Fagin like characters.
Both of these universes are real. We live in them every day. One is all upside, the other mostly down. We will have reached peak e-health the day that the downside exceeds the upside and stays there. Depending on who you are and what you read, for many clinicians, we have arrived at that point.
The laws of informatics
To understand why e-health often disappoints requires some perspective and distance. Informed observers again and again see the same pattern of large technology driven projects sucking up all the e-health oxygen and resources, and then failing to deliver. Clinicians see that the technology they can buy as a consumer is more beautiful and more useful that anything they encounter at work.
I remember a meeting I attended with Branko Cesnik. After a long presentation about a proposed new national e-health system, focusing entirely on technical standards and information architectures, Branko piped up: “Excuse me, but you’ve broken the first law of informatics”. What he meant was that the most basic premise for any clinical information system is that it exists to solve a clinical problem. If you start with the technology, and ignore the problem, you will fail.
There are many corollary informatics laws and principles. Never build a clinical system to solve a policy or administrative problem unless it is also solving a clinical problem. Technology is just one component of the socio-technical system, and building technology in isolation from that system just builds an isolated technology [3].
Breaking the laws of informatics
So, no e-health project starts in a vacuum of memory. Rarely do we need to design a system from first principles. We have many decades of experience to tell us what the right thing to do is. Many decades of what not to do sits on the shelf next to it. Next to these sits the discipline of health informatics itself. Whilst it borrows heavily from other disciplines, it has its own central reason to exist – the study of the health system, and of how to design ways of changing it for the better, supported by technology. Informatics has produced research in volume.
Yet today it would be fair to say that most people who work in the e-health space don’t know that this evidence exists, and if they know it does exist, they probably discount it. You might hear “N of 1” excuse making, which is the argument that the evidence “does not apply here because we are different” or “we will get it right where others have failed because we are smarter”. Sometimes system builders say that the only evidence that matters is their personal experience. We are engineers after all, and not scientists. What we need are tools, resources, a target and a deadline, not research.
Well, you are not different. You are building a complex intervention in a complex system, where causality is hard to understand, let alone control. While the details of your system might differ, from a complexity science perspective, each large e-health project ends up confronting the same class of nasty problem.
The results of ignoring evidence from the past are clear to see. If many of the clinical information systems I have seen were designed according to basic principles of human factors engineering, I would like to know what those principles are. If most of today’s clinical information systems are designed to minimize technology-induced harm and error, I will hold a party and retire, my life’s work done.
The basic laws of informatics exist, but they are rarely applied. Case histories are left in boxes under desks, rather than taught to practitioners. The great work of the informatics research community sits gathering digital dust in journals and conference proceedings, and does not inform much of what is built and used daily.
None of this story is new. Many other disciplines have faced identical challenges. The very name Evidence-based Medicine (EBM), for example, is a call to arms to move from anecdote and personal experience, towards research and data driven decision-making. I remember in the late ‘90s, as the EBM movement started (and it was as much a social movement as anything else), just how hard the push back was from the medical profession. The very name was an insult! EBM was devaluing the practical, rich daily experience of every doctor, who knew their patients ‘best’, and every patient was ‘different’ to those in the research trials. So, the evidence did not apply.
EBM remains a work in progress. All you need to do today is to see a map of clinical variation to understand that much of what is done remains without an evidence base to support it. Why is one kind of prosthetic hip joint used in one hospital, but a different one in another, especially given the differences in cost, hip failure and infection? Why does one developed country have high caesarian section rates when a comparable one does not? These are the result of pragmatic ‘engineering’ decisions by clinicians – to attack the solution to a clinical problem one way, and not another. I don’t think healthcare delivery is so different to informatics in that respect.
Is it time for evidence-based health informatics?
It is time we made the praxis of informatics evidence-based.
That means we should strive to see that every decision that is made about the selection, design, implementation and use of an informatics intervention is based on rigorously collected and analyzed data. We should choose the option that is most likely to succeed based on the very best evidence we have.
For this to happen, much needs to change in the way that research is conducted and communicated, and much needs to happen in the way that informatics is practiced as well:
- We will need to develop a rich understanding of the kinds of questions that informatics professionals ask every day;
- Where the evidence to answer a question exists, we need robust processes to synthesize and summarize that evidence into practitioner actionable form;
- Where the evidence does not exist and the question is important, then it is up to researchers to conduct the research that can provide the answer.
In EBM, there is a lovely notion that we need problem oriented evidence that matters (POEM) [1] (covered in some detail in Chapter 6 of The Guide to Health Informatics). It is easy enough to imagine the questions that can be answered with informatics POEMs:
- What is the safe limit to the number of medications I can show a clinician in a drop-down menu?
- I want to improve medication adherence in my Type 2 Diabetic patients. Is a text message reminder the most cost-effective solution?
- I want to reduce the time my docs spend documenting in clinic. What is the evidence that an EHR can reduce clinician documentation time?
- How gradually should I roll out the implementation of the new EHR in my hospital?
- What changes will I need to make to the workflow of my nursing staff if I implement this new medication management system?
EBM also emphasises that the answer to any question is never an absolute one based on the science, because the final decision is also shaped by patient preferences. A patient with cancer may choose a treatment that is less likely to cure them, because it is also less likely to have major side-effects, which is important given their other goals. The same obviously holds in evidence-based health informatics (EBHI).
The Challenges of EBHI
Making this vision come true would see some significant long term changes to the business of health informatics research and praxis:
- Questions: Practitioners will need develop a culture of seeking evidence to answer questions, and not simply do what they have always done, or their colleagues do. They will need to be clear about their own information needs, and to be trained to ask clear and answerable questions. There will need to be a concerted partnership between practitioners and researchers to understand what an answerable question looks like. EBM has a rich taxonomy of question types and the questions in informatics will be different, emphasizing engineering, organizational, and human factors issues amongst others. There will always be questions with no answer, and that is the time experience and judgment come to the fore. Even here though, analytic tools can help informaticians explore historical data to find the best historical evidence to support choices.
- Answers: The Cochrane Collaboration helped pioneer the development of robust processes of meta-analysis and systematic review, and the translation of these into knowledge products for clinicians. We will need to develop a new informatics knowledge translational profession that is responsible for understanding informatics questions, and finding methods to extract the most robust answers to them from the research literature and historical data. As much of this evidence does not typically come from randomised controlled trials, other methods than meta-analysis will be needed. Case libraries, which no doubt exist today, will be enhanced and shaped to support the EBHI enterprise. Because we are informaticians, we will clearly favor automated over manual ways of searching for, and summarizing, the research evidence [2]. We will also hopefully excel at developing the tools that practitioners use to frame their questions and get the answers they need. There are surely both public good and commercial drivers to support the creation of the knowledge products we need.
- Bringing implementation science to informatics: We know that informatics interventions are complex interventions in complex systems, and that the effect of these interventions vary depending on the organisational context. So, the practice of EBHI will of necessity see answers to questions being modified because of local context. I suspect that this will mean that one of the major research challenges to emerge from embracing EBHI is to develop robust and evidence-based methods to support localization or contextualisation of knowledge. While every context is no doubt unique, we should be able to draw upon the emerging lessons of implementation science to understand how to support local variation in a way that is most likely to see successful outcomes.
- Professionalization: Along with culture change would come changes to the way informatics professionals are accredited, and reaccredited. Continuing professional education is a foundation of the reaccreditation process, and provides a powerful opportunity for professionals to catch up with the major changes in science, and how those changes impact the way they should approach their work.
Conclusion
There comes a moment when surely it is time to declare that enough is enough. There is an unspoken crisis in e-health right now. The rhetoric of innovation, renewal, modernization and digitization make us all want to believers. The long and growing list of failed large-scale e-health projects, the uncomfortable silence that hangs when good people talk about the safety risks of technology, make some think that e-health is an ill-conceived if well intentioned moment in the evolution of modern health care. This does not have to be.
To avoid peak e-health we need to not just minimize the downside of what we do by avoiding mistakes. We also have to maximize the upside, and seize the transformative opportunities technology brings.
Everything I have seen in medicine’s journey to become evidence-based tells me that this will not be at all easy to accomplish, and that it will take decades. But until we do, the same mistakes will likely be rediscovered and remade.
We have the tools to create a different universe. What is needed is evidence, will, a culture of learning, and hard work. Less Dickens and dystopia. More Star Trek and utopia.
Further reading:
Since I wrote this blog a collection of important papers covering the important topic of how we evaluate health informatics and choose which technologies are fit for purpose has been published in the book Evidence-based Health Informatics.
References
- Slawson DC, Shaughnessy AF, Bennett JH. Becoming a medical information master: feeling good about not knowing everything. The Journal of Family Practice 1994;38(5):505-13
- Tsafnat G, Glasziou PP, Choong MK, et al. Systematic Review Automation Technologies. Systematic Reviews 2014;3(1):74
- Coiera E. Four rules for the reinvention of healthcare. BMJ 2004;328(7449):1197-99
An Italian translation of this article is available
The Forgetting Health System
October 7, 2015 § 2 Comments
Learning health systems are the next big thing. Through the use of information technology, the hope is that we can analyse all the data captured in electronic health records to speed both the process of scientific discovery and the translation of these discoveries into routine practice1,2. Every patient’s data, their response to treatment, and final outcome, will no longer be filed away, but feed the care of future patients3. It’s an exciting vision, and if we can achieve it, there is no doubt healthcare delivery would be transformed.
If we were to step back, we might conclude that although this is an admirable vision, for all its failings, the machinery of science is already working faster than we can handle it. The arena where organizational learning most needs to take hold is in the way we deliver health services. It is clear that we could do so much better in this arena. There is too much variation in patient care, too much waste and harm in the system.
So, if what we have today is not yet a learning health system, then by definition we must have the opposite – a forgetting health system. If that is the case, then here are two working definitions to contrast the two ideas:
- Learning system: The past shapes the future. Today’s mistake is tomorrow’s wisdom.
- Forgetting system: The past is the future. Today’s mistakes are forgotten quickly and are repeated tomorrow.
With this perspective it is easy to see examples everywhere of such ‘forgetting’. The history of large-scale e-health is a litany of the same case study being repeated. A large health IT project is started (usually by a government and usually as a technology innovation project rather than to fix a defined health problem). It quickly runs over time, over budget, and is treated with dismay as its users find it doesn’t do what they were promised. The end result is new problems, workarounds to circumvent the intruder technology, and in some cases, the eventual removal of the system.
The solution to this mess is of course seems to be to start a new large-scale e-health system, run by different people. Yet, like moths to a flame, these new protagonists seem to make the same set of strategic mistakes, but in new ways. Today’s large-scale health IT projects seem to be in a perpetual state of Groundhog Day, and must be a classic example of a forgetting system. This may be because there is no learning, because we convince ourselves that this time is ‘different’ and the past has nothing to teach us, or because when we look at past failures, we are unable to drawn any conclusions because of a lack of ability or imagination.
Information is lost
If a system ‘forgets’ then by implication that means that information that existed in the system has been lost, preventing its reuse to guide future events. If you think about it for one moment, the health system loses information every moment of every day, in unimaginable amounts. We only record a fraction of the events that occur. Most of these are not directly captured but rather are reconstructed from the memory of the individual making the record.
If we were to transform our forgetting system into a learning system, so that health system improvements are driven by experience, what do we need to do? For a system to ‘remember’ an event, a teachable moment, it firstly needs to be detected. You can’t remember what you never saw. Next, after detection, it needs to be recorded. Finally, this recording needs to be somehow aggregated with other events, for discovery of new knowledge to occur.
When it comes to treatment and diagnosis, we have built very precise mechanisms to detect important events or processes through a variety of diagnostic methods. The data captured are increasingly being recorded in electronic systems, and analysed. That’s the ‘big data’ movement in healthcare in a nutshell.
When it comes to health services, we still don’t know what events we should detect, what processes of service delivery should be instrumented, and there is still little thought to pooling system measurements in a way to allow across organizational analysis and learning. So, if we are to make our health services become learning ones, the task is much bigger than installing patient records.
One of the challenges to learning in health services is that, whilst it is easy to imagine that organizational memories can be stored in bits on a database, more often they will sit in the heads of those who work within them4. So, a good indicator that you are working in a forgetting system is that your organization has a high staff turnover – because it is very likely that when staff walk out the door they also walk with everything they know about the system that they are leaving, and no one has tried to capture that rich web of knowledge (if it could so easily be captured).
When learning also requires forgetting
Memories however also exist in other ways in an organisation. Crucially, they persist in the processes, protocols and built structures of the organisation, and in the workarounds and annotations that happen to physical spaces5. These structural memories are not inert or idly awaiting someone’s analysis. They sit there every moment shaping work, and altering human perceptions, actions and intent.
With time, accreted structural memories can lead to inertia, to an immovable status quo6. These kinds of memories therefore need to be managed. Some need to be revisited and revised, others are the jewels of the past that we should never forget and some, some are impeding the emerging purpose of an organization, and need to be actively forgotten. The need for organizational apoptosis, or active forgetting, is something I’ve written about before6.
From learning to adaptive systems
So, learning clearly is not nearly enough. Recording and analysing, at least as far as organisations are concerned, can only take you so far. The living walls and praxis of an organisation are already busy recording, even learning, but may not make it possible to do anything about what has been learned. For organisational inertia to be broken, and for repeated failures to be avoided, we not only need to learn, we need to actively, wisely, carefully, forget.
That will be a true learning system, because learning systems also need the capacity to change.
References
- Etheredge LM. A rapid-learning health system. Health affairs. 2007;26(2):w107-w118.
- Friedman CP, Wong AK, Blumenthal D. Achieving a nationwide learning health system. Science translational medicine. 2010;2(57):57cm29-57cm29.
- Gallego B, Walter SR, Day RO, et al. Bringing cohort studies to the bedside: framework for a ‘green button’ to support clinical decision-making. Journal of Comparative Effectiveness Research. 2015(0):1-7.
- Coiera E. When conversation is better than computation. Journal of the American Medical Informatics Association. 2000;7(3):277-286.
- Coiera E. Communication spaces. Journal of the American Medical Informatics Association. May 1, 2014 2014;21(3):414-422.
- Coiera E. Why system inertia makes health reform so hard. British Medical Journal. 2011;343:27-29.
A modest e-health proposal to government
May 12, 2015 § 4 Comments
Dear [insert country name] Government,
E-health is hard. I think we can all agree on that by now. You have spent [insert currency] [insert number] billion on e-health programs of one form or another over the last decade, and no one knows better than you how hard it is to demonstrate that you are making a difference to the quality, safety or efficiency of health care.
You also know that so much of e-health needs to happen in the public domain that, irrespective of your desire to privatise the problem, you will end up holding the can for much of what happens. E-health is your responsibility, and your citizens will, rightly or wrongly, hold you accountable.
It is so hard to get good strategic advice on e-health. You recently commissioned [insert large international consultancy firm] to prepare a new national e-health strategy, and it didn’t come cheap at [insert currency] [insert number] million. In the end it told you nothing you didn’t really already know, but at least you can say you tried.
You also commissioned [insert large international consultancy firm] to prepare a business case to back up that strategy, and it didn’t come cheaply either at [insert currency] [insert number] million. The numbers they came up with were big enough to convince Treasury to fund the national strategy, but deep in your heart of hearts you know you’ll never see a fraction of the [insert currency] promised.
It’s also really hard to find organisations that can deliver nation-scale e-health to time, to budget and of a quality that the professions and the voters all agree it’s a good thing. You want the IT folks who build these systems to understand health care, its needs and challenges, deeply. Just because they can build a great payroll system or website does not qualify them to jump in and manage an e-health project. Do you remember how [insert large IT company] ended up crashing and burning when they took on the [insert now legendary e-health project disaster]? We can all agree that didn’t go as planned, and that you didn’t exactly enjoy the coverage in the press and social media.
What you really want firstly is impartial, cheap and informed expert advice because you are in the end driven to do the right thing. Given the heated and partisan nature of politics, that advice needs to come from safe and trusted individuals. That often means the advice comes from within the tent of government, or from paid consultancies where legal contracts and the promise of future work secure your trust. You also want the IT folks who build your systems to be deeply trained in the complexities of implementing systems for e-health. The health professions, and indeed the voters, also need to be sophisticated enough to understand how to use these systems, and their limitations. That’s going to maximise your chances of success, as well as blunt the uninformed chatter that so often derails otherwise good policy.
Our proposal is a simple one. We suggest you set aside 10% of the E-health budget to train the next generation of e-health designers, builders, and users. Use the funds to resource training programs at the Masters level for future e-health policy leaders, as well as system designers, builders and implementers. Let us provide incentives to include e-health in health profession training both at primary degree and for continuing education. Let us also invest in training the public in the safe and effective use of e-health. Investing in creating a critical mass of skilled people over 5 years will be your best insurance that, when you are again faced with e-health, you have a real chance of doing the right thing.
Given how little outcome you have had for your e-health investments over the last decade, and the harsh reality that little will change over the next, this is a chance to rewrite the script. Invest in people and skills, and you might find that with time e-health isn’t so hard after all.
[insert name of concerned citizen, NGO, or professional association]
[insert date]
